Cushing Disease / Cushing Syndrome

The team at the OHSU Pituitary Center treats more than 250 patients at a time for Cushing disease/syndrome — a high number for such a rare illness. This condition is also known as hypercortisolism.
You can count on:
- Getting a precise diagnosis and a care plan tailored to your needs.
- Care from a team led by Dr. Maria Fleseriu, an internationally known neuroendocrinologist who specializes in Cushing disease/syndrome and a related condition, acromegaly.
- Skilled neurosurgeons who often use a minimally invasive approach to remove the pituitary tumors that cause Cushing disease.
- Sophisticated technology, including targeted radiation therapy.
- Leading researchers whose work led to FDA approval of medications for Cushing disease, and who are continuing innovative studies to improve care.
Learn more about:
Understanding Cushing disease and Cushing syndrome
What is Cushing disease?
Cushing disease (also called Cushing’s disease or hypercortisolism) occurs when your body makes too much cortisol, a hormone related to the body’s stress response. It’s a rare pituitary disorder that is progressive. That means that without treatment, it gets worse over time. With treatment, patients can lead active lives with fewer symptoms.
What’s the difference between Cushing syndrome and Cushing disease?
Both illnesses come from too much cortisol in the body.
In Cushing syndrome (also called Cushing’s syndrome), excess cortisol can come from outside or inside the body. For example, it can come from using corticosteroid medications, such as prednisone. Or it can come from a pituitary or adrenal tumor causing the body to make too much cortisol.
Cushing disease is a specific type of Cushing syndrome. It occurs when a pituitary tumor causes the body to make too much cortisol. Cushing disease is the most common form of endogenous (from the body) Cushing syndrome, and makes up about 70% of Cushing syndrome cases.
Who gets Cushing disease/syndrome?
- Incidence: Cushing disease/syndrome is rare. About 10 to 15 new cases per million people are diagnosed in the U.S. each year. These numbers may not reflect the true number of people with this illness, though, because it’s not uncommon for people to go undiagnosed.
- Age: It is typically found in people ages 20 to 50.
- Sex: It affects roughly three times as many women as men.
What causes Cushing disease?
Cushing disease occurs when a pituitary adenoma, a noncancerous (benign) tumor on the pea-size pituitary gland, makes too much adrenocorticotropic hormone (ACTH).
In response, the body’s two adrenal glands, one atop each kidney, make too much cortisol. This causes problems with your body’s hormone balance.
Only about 10% of pituitary adenomas make too much ACTH. The tumor can also be small (microadenoma) or large (macroadenoma).
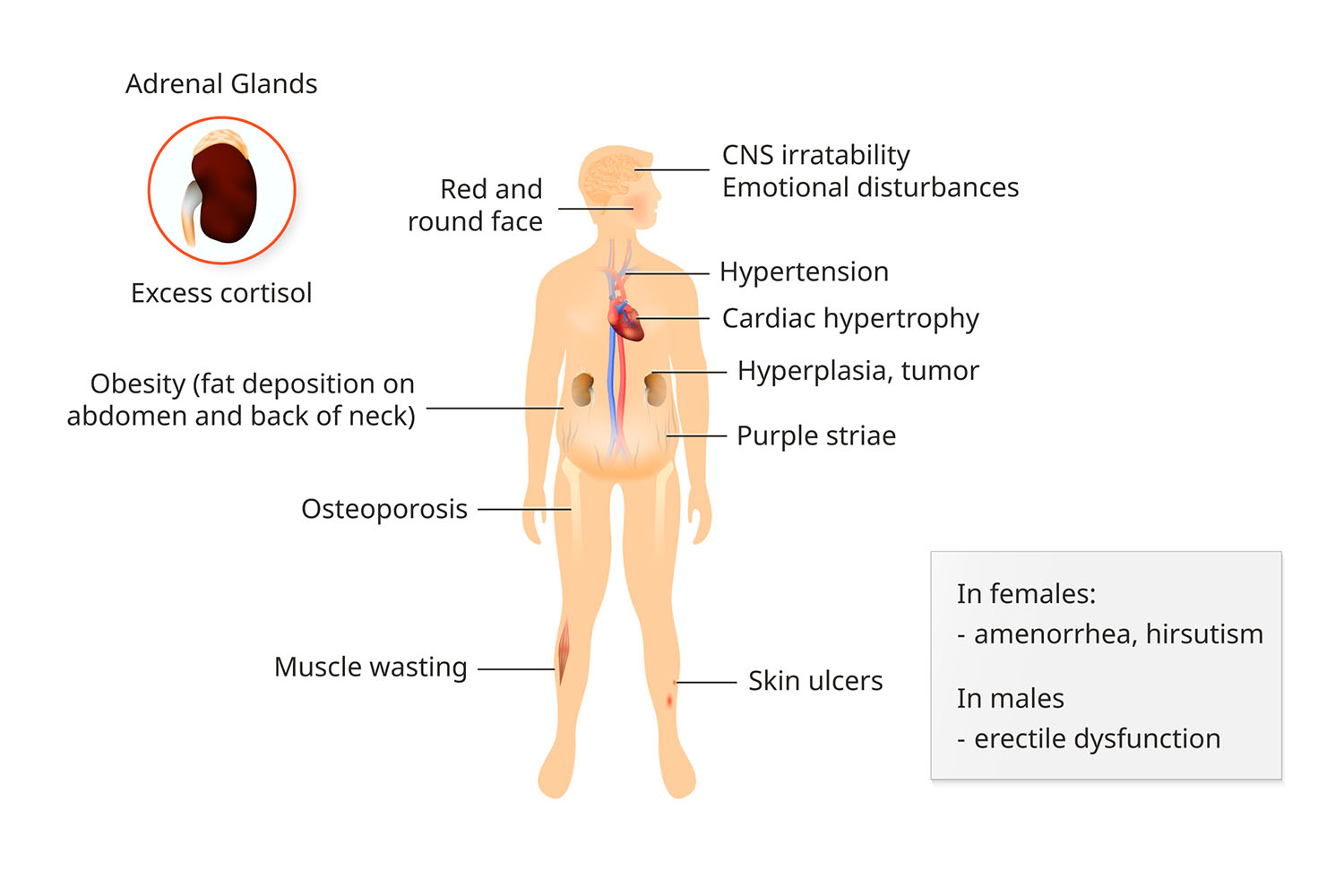
Symptoms and complications of Cushing disease/syndrome
Cushing disease/syndrome can change your appearance. Signs include:
- Round, red face
- Hump on back of neck
- Purple stretch marks, especially on the chest, armpits and belly
- Skin changes, such as acne, excessive facial hair and easy bruising
- Unusual, rapid weight gain, especially around the belly
Complications can include:
- Muscle weakness
- Vision problems
- Headaches
- Infections
- Osteoporosis, a condition that causes weak, brittle bones and bone loss
- High blood pressure
- High blood sugar or diabetes
- Extreme fatigue or trouble sleeping
- Depression
- Memory loss
- In women, loss of periods (amenorrhea), and male-pattern face and body hair (hirsutism)
- In men, trouble getting an erection
Cushing Syndrome Symptoms
Diagnosing Cushing disease/syndrome
Cushing disease/syndrome can be challenging to diagnose because changes can happen slowly. It’s not uncommon for us to see patients who have gone undiagnosed or who have been misdiagnosed for years. Because we’ve treated hundreds of patients with Cushing disease or syndrome, we have the skills to give you the right diagnosis so you can begin treatment.
We start with a full exam to:
- Rule out other disorders: Your symptoms may be related to another condition. We first need to confirm whether symptoms are linked to elevated ACTH and cortisol.
- Find the source of the extra hormones: We’ll do tests to see if your disease is:
- ACTH dependent: Caused by a pituitary tumor or, rarely, a tumor in another part of the body.
- ACTH-independent: Caused by overactive adrenal glands or an adrenal tumor.
- Trace possible causes: Your doctor will ask you if you use or have recently used steroid medications, creams or inhalers that contain hydrocortisone, prednisone or dexamethasone. Your doctor will also ask about use of birth control pills. We may ask you to switch to a different type of birth control during testing.
Screening tests for Cushing disease/syndrome
- Blood tests: We can measure the levels of ACTH and cortisol in your blood. We take a blood sample in the morning because hormone levels change throughout the day.
- Urine tests: We can measure cortisol in your urine. We may ask for multiple samples. Ask your doctor if any of your current medications could affect results.
- Late-night saliva test: We look at cortisol in your saliva. You’ll collect several samples just before midnight, when cortisol usually drops to its lowest level. A high level can indicate Cushing disease/syndrome.
Imaging tests for Cushing disease/syndrome
- MRI: This scan can help us see a pituitary tumor, including its size and location. If you’ve had an MRI before coming to us, we’ll recommend a new one only if the other scan was inconclusive. Sometimes pituitary tumors aren’t visible.
- Abdominal CT scan: We’ll recommend this scan only if we think it’s possible you have an adrenal tumor. The scan can show a tumor, some of its features, and which side it’s on.
Confirming a Cushing diagnosis
Dexamethasone suppression/corticotropin-releasing hormone stimulation test (DEX/CRH):
If screening tests show high ACTH/cortisol levels, we may use this blood test to confirm the diagnosis. We give you medications to lower or raise certain hormones. This helps us see if symptoms are from Cushing disease/syndrome or a condition such as depression, stress, kidney failure or alcoholism.
Inferior petrosal and cavernous sinus sampling: If tests indicate that high ACTH is causing Cushing, we’ll find out if the problem is from your pituitary gland or some other part of your body (ectopic Cushing syndrome). We’ll insert thin tubes called catheters into areas (sinuses) alongside your pituitary gland. We’ll monitor your ACTH levels during the test. If your pituitary gland is the source, we’ll arrange for you to consult with a neurosurgeon. For ectopic Cushing syndrome, we’ll work with other OHSU specialists for further treatment.
Cushing disease/syndrome treatments
Treatment for Cushing disease/syndrome has changed in the last decade, thanks to several breakthroughs for treating pituitary adenomas with medication.
The OHSU Pituitary Center was one of the leading contributors to clinical trials that led to medications — pasireotide and mifepristone — to treat Cushing disease/syndrome and acromegaly.
Surgery
Surgery to remove a tumor causing the problem is often the first treatment for Cushing disease. At a specialized pituitary center such as ours, surgery to remove a small pituitary tumor has a success rate of 80-85%.
We use a precise, minimally invasive procedure called transsphenoidal surgery to remove pituitary tumors through the nose. This approach leaves no visible external scars and has few side effects and risks. You will most likely go home two or three days after surgery.
Medication
For some patients, surgery isn’t an option or doesn’t fully solve the problem. You may need medication for Cushing disease/syndrome:
- Before surgery to control cortisol levels.
- If you can’t have surgery because of other health reasons or risks.
- If you had surgery, but the neurosurgeon couldn’t remove the entire tumor or the removal didn’t solve the problem.
- If you have too much ACTH, but a tumor doesn’t show up on imaging.
Some patients may need a combination of medications. All drugs used for Cushing disease/syndrome can potentially cause adrenal insufficiency, or a low level of adrenal hormones. This can cause fatigue and muscle weakness, among other symptoms. Our team will monitor you closely and provide treatment if this happens.
Medications for Cushing disease/syndrome include:
- Central-acting inhibitors of ACTH: Pasireotide (a somatostatin receptor ligand, or SRL) reduces ACTH to normal levels for about a quarter of patients. It lessens symptoms for others. Most see results within two months. This medication is injected and can cause side effects, including high blood sugar and diabetes, in more than half of patients. Your doctor will talk with you about risks and benefits.
- Adrenal-directed inhibition of steroidogenesis: Medications in this category are used off-label for Cushing disease. This means the doctor uses a safe and FDA-approved medication for a reason other than its approved use. Our team has extensive experience with off-label uses for Cushing disease. Medications include ketoconazole, metyrapone, mitotane and etomidate. They target the adrenal glands to lower cortisol levels.
- Glucocorticoid receptor blockade: OHSU participated in the clinical trial that led to FDA approval for this medication, called mifepristone. It’s used to treat high blood sugar associated with Cushing syndrome. Mifepristone may improve other conditions brought on by too much cortisol. It can also cause low potassium levels, called hypokalemia, and vaginal bleeding. It’s not recommended for women who wish to become pregnant.
Radiation therapy
Some patients have an aggressive form of Cushing disease, and surgery and medication don’t help. In these cases, we may recommend a type of targeted radiation therapy called stereotactic radiosurgery to control hormone levels.
We use the most advanced equipment available, the Novalis Tx radiosurgery system. This lets us shape the radiation beam to match the tumor while sparing healthy tissue.
Medication and radiation therapy: Most patients who have had radiation therapy have medication for an extended period. We stop the medication, usually once a year, to see if the radiation worked.
Follow-up care
After surgery and if you are in remission, your body no longer produces cortisol. You will need medication to maintain normal levels. Symptoms can take time to go away. During this time, you’ll receive follow-up care from our experts.
Cushing disease comes back, even after decades, in about a quarter of cases. We will monitor you closely and recommend further treatment if needed.
Learn more
- Cushing’s Syndrome, National Institute of Diabetes and Digestive and Kidney Diseases
- Cushing disease, U.S. National Library of Medicine
- Cushing Syndrome, Eunice Kennedy Shriver National Institute of Child Health and Human Development
- Cushing’s Syndrome/Disease, American Association of Neurological Surgeons
For patients
- Referral: To become a patient, please ask your doctor for a referral.
- Questions: For questions or follow-up appointments, call 503-494-4314.
Location
Parking is free for patients and their visitors.
OHSU Pituitary Center
Center for Health & Healing Building 1
3303 S. Bond Ave.
Portland, OR 97239
Map and directions
Refer a patient
- Refer your patient to OHSU.
- Call 503-494-4567 to seek provider-to-provider advice.
- See more pituitary information for health care professionals.
- OHSU Provider’s Guide to Pituitary Disorders