Projects
Right heart growth in the functionally univentricular fetus
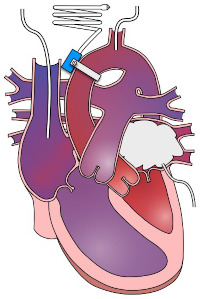
The left side of the heart pumps blood to the body, but sometimes it doesn't grow in the fetus. When that happens, the heart depends on the right side to do all the work. The right side of the heart is important for pumping blood to the lungs after birth, but before birth it pumps blood to the body with the left side. At birth, infants with the this anatomical defect of reduce left sided heart growth (a functionally univentricular heart) require a series of life-saving surgeries. However, the right side of the heart is intrinsically different than the left, and responds differently to a lifetime of the work of pumping blood to the body instead of the lungs. Individuals with this "hypoplastic" left heart are at increased risk of heart failure.
We are interested in how the additional work in fetal life changes how the right ventricle grows in this condition. Does it stimulate growth of more of the muscle cells of the heart ("cardiomyocytes") or does it cause them to mature earlier and make less of themselves? Do the cells grow larger? How do these right ventricles function? And what are the consequences to the organs receiving blood in fetal life? We are using fetal sheep to answer these questions to advance our ability to help families facing these congenital defects.
Publications:
-
Onohara D, Hagen M, Louey S, Giraud G, Jonker S, and Padala M. Chronic in utero mitral inflow obstruction unloads left ventricular volume in a novel late gestation fetal lamb model. JTCVS Open 16: 698-707, 2023.
-
Hagen M, Louey S, Alaniz SM, McClellan E, Lidner JR, Giraud GD, Jonker SS. Enhanced myocardial perfusion in late gestation fetal lambs with impaired left ventricular inflow. J Physiol 4 January 2025. doi.org/10.1113/JP286685.
The number of muscle cells in the heart at birth

The number of muscle cells in the heart ("cardiomyocytes") contribute to the strength and resilience of the heart. Some of these cells die as we get older. They also die when the heart is stressed. The total number of cardiomyocytes decreases with aging because new cells are made very slowly after birth. Because of that, it is very important how many cardiomyocytes you have at birth. This is especially true if you have heart disease, including congenital heart disease. How you grow as fetus and infant has been shown to affect your life-long risk of disease!
To increase heart health, keeping cardiomyocyte number high is important. Doctors prescribe therapies to reduce the number of cardiomyocytes that die. Scientists are working very hard to find ways to restore cardiomyocyte number through stem cell therapy. We have discovered that right before birth, a lot of cardiomyocytes die all at once. Now we are trying to find ways to stop this loss of cardiomyocytes. Because we can't study the muscle cells in the hearts of human babies, we are using sheep to understand why these cardiomyocytes die, and what we can do to save them.
Publications:
- Bose K, Espinoza HM, Louey S, and Jonker SS. Sensitivity and activation of endoplasmic reticulum stress response and apoptosis in the perinatal sheep heart. Am J Physiol Heart Circ Physiol 327: H1-H11, 2024.
How the fetal heart responds to fat
Fetuses get all of their nutrition from mom through the placenta. The level of fat in fetal blood is usually low. Instead of fat, hearts of fetuses mostly use carbohydrate such as glucose and lactate for energy. But after birth, babies starts nursing fatty milk. The fat levels in the baby's blood increase. The heart of a baby uses a lot of fat for energy. The machinery of the heart muscle cells ("cardiomyocytes" needs to change in order for the cells to switch from using carbohydrates to using fat. High levels of fat can kill immature fetal cardiomyocytes. But the machinery in these cells is ready for fats even before birth. How does the heart know to prepare? We are working to understand when and how the cardiomyocytes stop being sensitive to fat, and instead learn to use it for energy.
Publications:
- Chattergoon N, Louey S, Jonker SS, and Thornburg K. Thyroid hormone increases fatty acid use in fetal ovine cardiac myocytes. Physiol Rep 11: e15865, 2023.
- Piccolo BD, Chen A, Louey S, Thornburg KLR, and Jonker SS. Physiological response to fetal intravenous lipid emulsion. Clin Sci (Lond) 138: 117-134, 2024.
The connection between muscle cell growth and capillary growth
Muscle cells use a lot of energy to do their work. Blood provides the nutrients and oxygen they need, and remove their waste. This nutrient exchange happens between muscle cells and the very smallest blood vessels ("capillaries"). When muscle cells don't get enough blood, they stop contracting as well, they become resistant to insulin (pre-diabetic), and they get sick and die. How the capillaries grow in the fetus and baby has been shown to affect life-long risk of these problems!
But when fetal environment or health changes heart muscle growth, how does that change capillary growth to the heart? How does that new relationship persist, or resolve? These questions will help us understand the developmental origins of coronary health and disease.
Publications:
- Hagen MW, Louey S, Alaniz SM, Brown L, Lindner JR, and Jonker SS. Coronary conductance in the normal development of sheep during the perinatal period. Physiol Rep 10: e15523, 2022.
- Hagen MW, Louey S, Alaniz SM, Belcik T, Muller MM, Brown L, Lindner JR, and Jonker SS. Changes in microvascular perfusion of heart and skeletal muscle in sheep around the time of birth. Exp Physiol 108: 135-145, 2023.