How can we improve the evaluation and care of patients with glaucoma? Glaucoma is one of the leading causes of legal blindness, and affects about six percent of adult Americans. It has an even higher prevalence in Black and Latinx populations. As glaucoma is asymptomatic until its advanced stages, it is common that severe disease happens more often in groups that have limited access to eye care. Half of the patients with glaucoma in the U.S remain undiagnosed.
The Covid-19 pandemic provides an interesting insight into how we might establish a population-based approach to address glaucoma and find that other half of patients who remain undiagnosed. During the past two years, restrictions on in person visits changed how we use many types of technology to provide ongoing care of patients with glaucoma.
Researchers and doctors at Casey have focused their efforts to provide the framework for expanding this change in patient care to provide improved screening, diagnosis and care of patients with glaucoma.
At the forefront of early glaucoma diagnosis
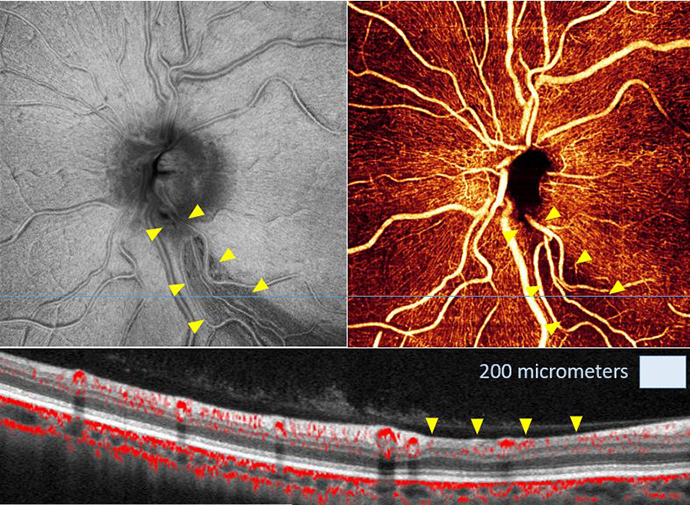
First of all, researchers with Casey’s Center for Ophthalmic Optics and Lasers (COOL lab) demonstrated that the non-invasive imaging technology OCT angiography is a reliable way to detect glaucoma early by viewing blood vessels in the eye. OCT angiography could be a technology we are able to use to screen many people for the unsuspected presence of glaucoma.
Secondly, Casey researchers are also developing artificial intelligence algorithms for looking at eye images to recognize those patients with glaucoma. This is another way doctors can detect glaucoma early in large populations.
Finally, The Roundhouse Foundation has provided funding to implement this approach in pilot sites throughout Oregon. By making a diagnosis early in patients without symptoms, many who lack easy access to quality eye care, we will have the best chance of reducing the prevalence of vision loss from glaucoma in Oregon and beyond.
Getting it right
The evolution of the way we diagnose and care for glaucoma requires careful study, and Casey’s team of leading experts are working together to conduct just such an analysis. David Huang, M.D., Ph.D., and Yali Jia, Ph.D., in the COOL lab will provide unparalleled expertise in imaging. Michelle Hribar, Ph.D., and Hiroshi Ishikawa, M.D., Ph.D., will develop artificial intelligence processing applications. Finally, the Casey Community Outreach Program, led by Mitchell Brinks, M.D., M.P.H., and Verian Wedeking, is building a network of community health workers in Oregon to support the implementation of this approach in high risk populations.
Casey’s glaucoma division has embraced this project, and Aiyin Chen, M.D., one of Casey’s glaucoma specialists, will be evaluating whether these tools and technologies can be successful in early glaucoma screening and detection.